
Malaria is a life-threatening disease caused by protozoan parasites of the genus Plasmodium. The disease is transmitted to humans through the bite of infected female Anopheles mosquitoes. There are five species of Plasmodium that commonly infect humans: Plasmodium falciparum, P. vivax, P. malariae, P. ovale, and P. knowlesi. Among these, P. falciparum is the most deadly, responsible for the majority of severe cases and deaths, particularly in sub-Saharan Africa. P. vivax is the most widespread and can cause relapsing malaria due to dormant liver stages called hypnozoites. The life cycle of Plasmodium involves both human and mosquito hosts, with complex stages including liver infection (exoerythrocytic) and red blood cell infection (erythrocytic).
Malaria remains one of the world’s most pressing public health issues.
As of 2024, malaria continues to pose a significant global health challenge, with the disease remaining prevalent, particularly in low-income regions. In 2022, an estimated 249 million cases of malaria were reported globally, resulting in approximately 608,000 deaths. The burden of the disease is heavily concentrated in the WHO African Region, which accounted for 94% of all cases and 95% of deaths. This region remains disproportionately affected, with young children and pregnant women among the most vulnerable groups.
Children under five years of age are particularly at risk, comprising 78% of malaria-related deaths in the African Region. The disease’s prevalence in these areas is exacerbated by challenges such as limited access to healthcare, inadequate vector control measures, and socioeconomic factors.
Despite ongoing efforts to control and eliminate malaria, progress has been uneven. Factors like resistance to antimalarial drugs and insecticides, as well as environmental changes, complicate eradication efforts. The economic impact of malaria is also substantial, affecting the productivity and development of affected countries.
Global initiatives continue to focus on improving preventive measures, enhancing access to treatment, and addressing the socioeconomic determinants of health that contribute to the persistence of malaria. These efforts are crucial in striving toward a more equitable world where the burden of malaria is significantly reduced.
Malaria has afflicted humans for millennia, with its presence documented in various ancient civilizations. The disease’s impact on history is profound, influencing not only the health but also the culture, economy, and warfare of ancient societies.
In Ancient Egypt, references to malaria-like symptoms are found in medical texts such as the Ebers Papyrus (circa 1550 BCE), one of the oldest medical documents. The Egyptians attributed the disease to the influence of evil spirits and sought to treat it with various herbal remedies. The condition was described as “heating of the head,” indicative of fever, a common symptom of malaria.
Chinese records also provide early descriptions of malaria. The Nei Ching (The Canon of Medicine), attributed to the Yellow Emperor and dating back to 2700 BCE, mentions intermittent fevers. This ancient medical text outlines treatments using qinghao (Artemisia annua), a plant later identified as a source of artemisinin, a key compound in modern antimalarial drugs.
In Mesopotamian civilization, cuneiform tablets from as early as 2000 BCE contain descriptions of ailments characterized by chills and fever, which are consistent with malaria symptoms. The Assyrians and Babylonians believed these fevers were caused by demons and sought cures through prayers and rituals.
Malaria was also well-known in Ancient Greece, where it significantly impacted the health and lives of the population. The Greek physician Hippocrates (460–370 BCE) documented the symptoms of malaria, distinguishing between the different forms of fever patterns, such as tertian (fever every third day) and quartan (fever every fourth day), which correspond to infections caused by Plasmodium vivax and Plasmodium malariae, respectively.
In Rome, malaria had a profound impact on the city’s development. The disease was rampant in the marshes around Rome, which were later known as the Pontine Marshes. Malaria was referred to as “Roman fever,” and its prevalence was thought to contribute to the decline of the Roman Empire by debilitating the population and military. The term “malaria” itself comes from the Italian words “mala aria,” meaning “bad air,” a reference to the mistaken belief that the disease was caused by foul air from swamps.
Malaria was also present in other ancient civilizations, including the Indian subcontinent, where it was described in Ayurvedic texts. The Sushruta Samhita, an ancient Sanskrit text, mentions the symptoms of intermittent fever, known locally as “vishama jwara.”
The history of malaria research is marked by several key scientific discoveries that have significantly advanced our understanding of the disease and its management. Here are some of the most important milestones:
The life cycle of Plasmodium parasites involves several stages that take place in two different hosts:
Malaria symptoms can range from mild to severe, depending on several factors such as the Plasmodium species involved, the individual’s immune status, and access to timely treatment. Chronic malaria occurs when a person remains infected with malaria parasites for an extended period, often lasting months or even years.
The malaria eradication campaigns of the 1950s and 1960s were part of a global effort aimed at reducing and ultimately eliminating malaria, a deadly and widespread infectious disease caused by Plasmodium parasites transmitted by Anopheles mosquitoes. These campaigns were driven by advancements in medical knowledge, public health strategies, and international cooperation.
Challenges and Limitations:
Program Conclusion and Legacy:
The malaria eradication campaigns of the 1950s and 1960s provided valuable lessons in public health, particularly in the importance of sustained political and financial commitment, the challenges of developing resistance, and the need for adaptable and comprehensive strategies. These lessons continue to inform current global efforts to combat malaria, with a renewed focus on integrated approaches that include vector control, effective treatment, vaccine development, and robust health systems.
The landscape of malaria diagnostics has evolved significantly, from traditional microscopy to advanced molecular techniques and emerging technologies. Each diagnostic tool has its advantages and limitations, making them suitable for different contexts. While microscopy remains a standard method due to its high specificity and ability to estimate parasite density, RDTs offer rapid and user-friendly options for field settings. PCR and LAMP provide high sensitivity and accuracy, particularly for low parasitemia and species identification, but require more complex infrastructure. Emerging technologies, including nanotechnology and AI, hold promise for future advancements in malaria diagnostics. The continued development and integration of these tools are crucial for effective malaria control and eradication efforts. Malaria diagnistic tools include:
Before modern antimalarials, malaria was treated with various traditional remedies. One of the earliest and most effective treatments was the bark of the Cinchona tree, which contains quinine. Indigenous people in South America used this bark to treat fevers, a practice later adopted by Europeans in the 17th century. Quinine became the first successful treatment for malaria and remained the primary antimalarial until the 20th century. Other historical remedies included the use of the Chinese herb Artemisia annua, which contains artemisinin, a compound now central to modern antimalarial therapies. Additionally, ancient Egyptians and Greeks used herbal concoctions, and the Romans recognized the importance of draining swamps to reduce mosquito populations.
Cinchona Bark in Europe:
Advancements in Quinine Production:
Synthetic Drug Development:
Primaquine and Comprehensive Treatment:
Resistance Development:
Combination Therapies:
Modern-day malaria treatments focus primarily on the use of antimalarial drugs, with Artemisinin-based Combination Therapies (ACTs) being the cornerstone of treatment for Plasmodium falciparum malaria, the most severe form of the disease. The shift to ACTs as the first-line treatment emerged due to the increasing prevalence of drug-resistant malaria parasite strains.
Artemether-Lumefantrine (Coartem): One of the most widely used ACTs, typically administered as a six-dose regimen over three days. It is effective against drug-resistant P. falciparum.
Artesunate-Mefloquine: Commonly used in Southeast Asia, where it remains highly effective despite concerns about mefloquine resistance.
Artesunate-Amodiaquine: Often used in Africa and recommended in many national treatment guidelines.
Dihydroartemisinin-Piperaquine: Notable for its longer half-life, which offers the advantage of a simpler dosing regimen (typically once daily for three days).
Artemether-Benflumetol (Lumefantrine): Another formulation of artemether-lumefantrine.
Malarone, a combination of atovaquone and proguanil, is a widely used antimalarial medication in modern-day interventions. It is effective for both the prevention and treatment of malaria. Atovaquone disrupts the mitochondrial electron transport chain in the parasite, specifically inhibiting the cytochrome bc1 complex. This action leads to the collapse of mitochondrial membrane potential and disruption of ATP synthesis, ultimately killing the parasite. Proguanil is a prodrug that is converted in the body to its active form, cycloguanil. Cycloguanil inhibits dihydrofolate reductase (DHFR), an enzyme crucial for folate synthesis in the parasite, impairing DNA synthesis and cell division. The combination of atovaquone and proguanil works synergistically to effectively clear parasitemia.
Prophylaxis (Prevention):
Treatment of Acute Malaria:
Malarone remains an important tool in the prevention and treatment of malaria, particularly for travelers and in regions with drug-resistant P. falciparum. Its effectiveness, tolerability, and user-friendly dosing schedule make it a preferred choice for many, despite considerations around cost and potential resistance. Its role in modern antimalarial interventions continues to be significant, contributing to the global effort to control and eventually eradicate malaria.
Quinine has a long history of use in the treatment of malaria. Although its use has declined with the advent of more effective and better-tolerated medications, itstill plays a crucial role in certain clinical situations, particularly for severe malaria or when other treatments are not available or suitable. Quinine works by interfering with the parasite’s ability to metabolize hemoglobin, leading to the accumulation of toxic heme within the parasite’s food vacuole, which ultimately kills the parasite.
Treatment of Severe Malaria:
Oral Quinine for Uncomplicated Malaria:
Side Effects and Monitoring:
Quinine, though largely superseded by newer treatments, remains an important drug in the global fight against malaria, particularly in severe cases or where newer therapies are unavailable. Its use requires careful medical supervision due to potential side effects and the need for specific dosing and monitoring protocols. Its historical significance and continued utility in certain scenarios underscore its role in the history and ongoing management of malaria.
The history of funding for malaria control and research reflects a complex interplay of scientific advancements, public health priorities, global economic conditions, and geopolitical factors. This timeline provides an overview of key phases and milestones in the history of malaria funding.
Funding for malaria remains critical, with international donors, national governments, and private foundations playing key roles. The Global Fund, PMI, and the Gates Foundation continue to be major contributors. There is a growing emphasis on domestic funding and innovative financing mechanisms to ensure long-term sustainability.
Addressing both scientific and non-scientific challenges is crucial for the effective control and eventual eradication of malaria. A multidisciplinary approach involving medical research, public health policy, education, and community engagement is necessary to overcome these barriers and make substantial progress in the fight against malaria.
Drug Resistance:
Insecticide Resistance:
Complexity of the Parasite’s Life Cycle:
Limited Vaccine Efficacy:
Diagnostic Challenges:
Socioeconomic Factors:
Political and Economic Instability:
Healthcare Infrastructure:
Cultural and Behavioral Factors:
Funding and Resource Allocation:
Climate Change and Environmental Factors:
Several Nobel Prizes have been awarded for research related to malaria, highlighting the significance of scientific discoveries in understanding and combating this disease:
Artemisia annua.
The term “scourge of humanity” in relation to malaria captures the disease’s extensive historical impact, its severe health and socioeconomic consequences, and the ongoing challenges it presents. Malaria continues to be a significant global health challenge, affecting millions of people annually and causing considerable morbidity and mortality. While substantial progress has been made in understanding the disease, improving diagnostics and treatment, and developing control measures, significant challenges remain. Ongoing research, international collaboration, and sustained commitment are essential to overcoming these challenges and ultimately achieving the goal of malaria elimination and eradication.
Malaria Site – http://www.malariasite.com/
Malaria.com – http://www.malaria.com/
World Health Organization – http://www.who.int/topics/malaria/en/
Center for Disease Control – http://www.cdc.gov/MALARIA/
The Global Fund – https://www.theglobalfund.org/en/malaria/
National Institutes of Health – http://health.nih.gov/topic/Malaria
National Institute of Allergy and Infectious Diseases – http://www.niaid.nih.gov/topics/malaria/Pages/default.aspx
National Health Services – https://www.nhs.uk/conditions/malaria/
Bill & Melinda Gates Foundation – http://www.gatesfoundation.org/topics/pages/malaria.aspx
Roll Back Malaria Partnership to end Malaria – http://www.rbm.who.int/
Malaria No More – https://www.malarianomore.org/
Malaria Vaccine Initiative – https://www.path.org/who-we-are/programs/center-for-vaccine-innovation-and-access/delivering-malaria-vaccines/
Medicines for Malaria Venture – http://www.mmv.org/
PlasmoDB – https://plasmodb.org/plasmo/app
BEI Resources – https://www.beiresources.org/
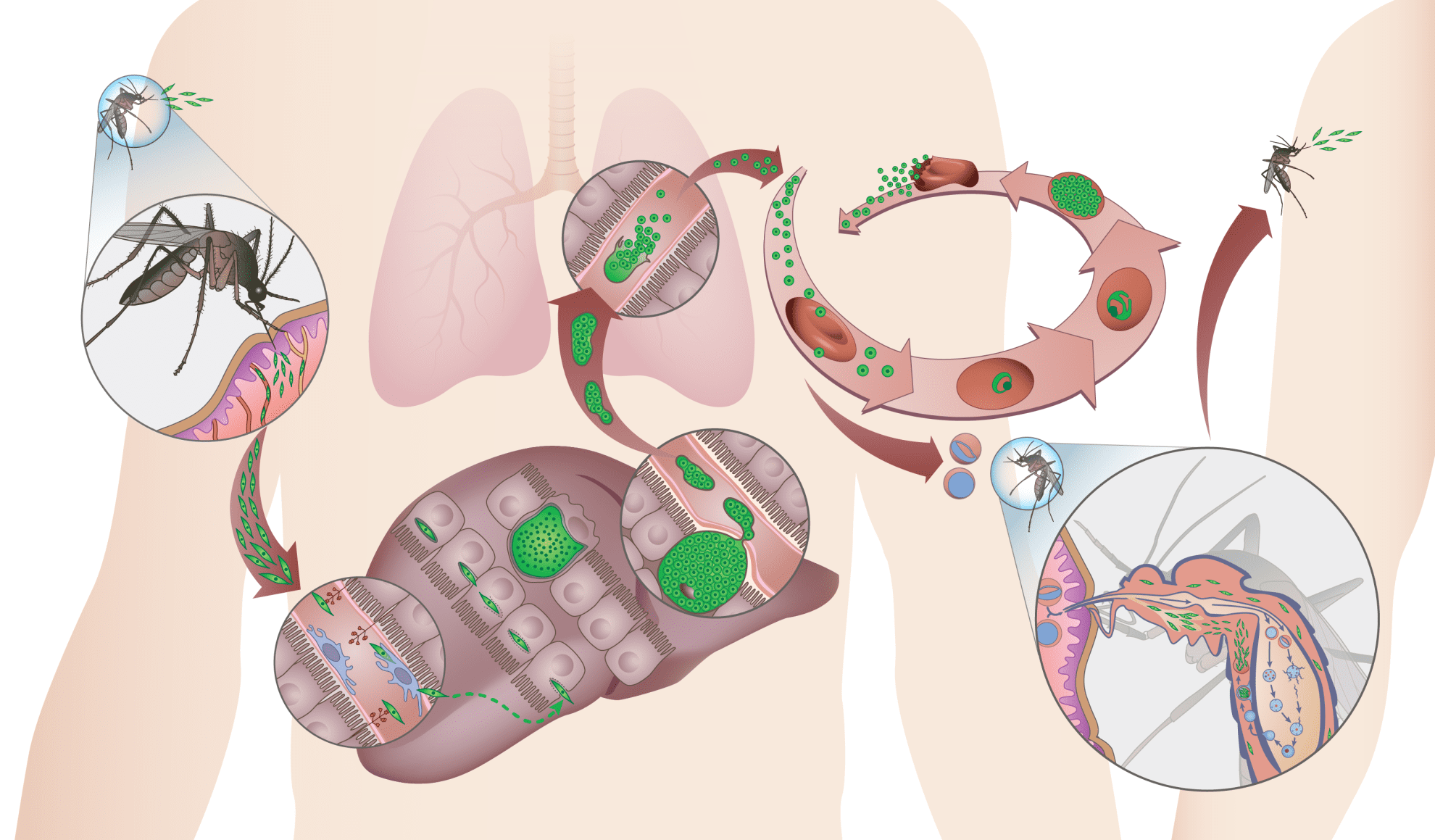
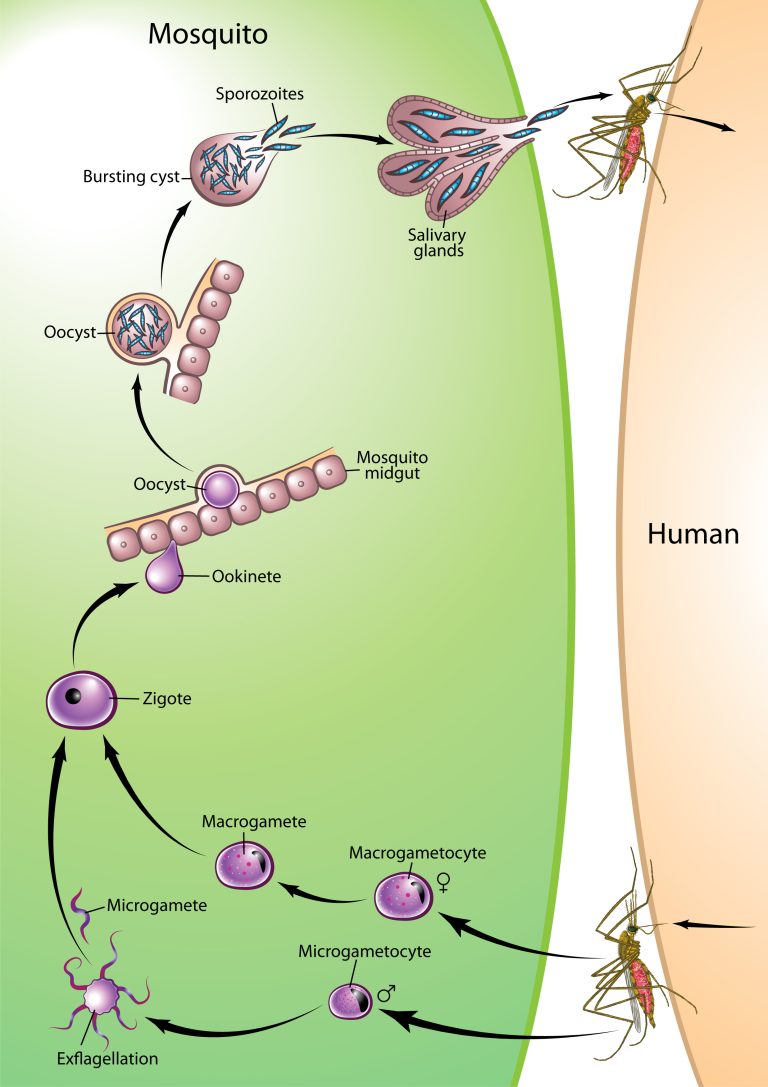
Infection by malaria parasites is initiated when Plasmodium sporozoites enter the mammalian host through the bite of an infected female Anopheles mosquito. Sporozoites deposited under the skin during a blood meal migrate to the liver, where traverse a few hepatocytes and eventually productively invade one, with formation of a parasitophorous vacuole. Inside this vacuole, the parasites replicate extensively and develop into merozoites, which are eventually released into the bloodstream. Each merozoite will invade an erythrocyte, initiating a replication cycle that ends with the release of new merozoites from the mature infected erythrocyte (schizont), which go on to infect other erythrocytes. Malaria- associated pathology only occurs during the blood stage of infection. The Plasmodium life cycle continues when some parasite blood stages develop into the sexual parasite stages, the male and female gametocytes, which can be taken up by mosquitoes during blood meals. Gametocytes undergo fertilization and maturation in the mosquito midgut, forming an infective ookinete form that migrates through the mosquito midgut into the hemocele, developing into the oocyst, in which sporozoites are formed. When fully matured, the oocysts burst and release sporozoites, which migrate into the mosquito’s salivary glands, ready for the next transmission step.
Anopheles mosquitoes go through four separate and distinct stages of its life cycle which are as follows: egg, larva, pupa, and adult. Each of these stages can be easily recognized by their special appearance. Female Anopheles mosquitoes lay their eggs singly on the water. Larvae live in the water and come to the surface to breathe. They shed their skin four times growing larger after each molting. Anopheles larvae lie parallel to the water surface and feed on micro-organisms and organic matter in the water. On the fourth molt the larva changes into a pupa. Pupae are a resting, non-feeding stage. This is the time the mosquito turns into an adult. It takes about two days before the adult is fully developed. When development is complete, the pupal skin splits and the mosquito emerges as an adult. Adults rest on the surface of the water for a short time to allow themselves to dry and all of their parts to harden. Also, the wings have to spread out and dry properly before they can fly.

Plasmodium is a genus of parasitic protozoa that causes malaria in various vertebrate hosts. The genus includes numerous species, each adapted to specific hosts, ranging from humans and other mammals to birds, reptiles, and amphibians. Here is a comprehensive list of known Plasmodium species, categorized by their respective vertebrate hosts, including both well-documented and lesser-known species across various vertebrate classes:
There are over 460 recognized species within the genus Anopheles. Not all species are equally important in the transmission of malaria; some are major vectors, while others may only occasionally transmit the disease or not at all. Additionally, vector competence can vary widely within species due to genetic, environmental, and ecological factors. This list provides an overview of some key Anopheles species ordered roughly by their significance in malaria transmission.
{kind=link}
{kind=link}