Vaccines against Plasmodium falciparum
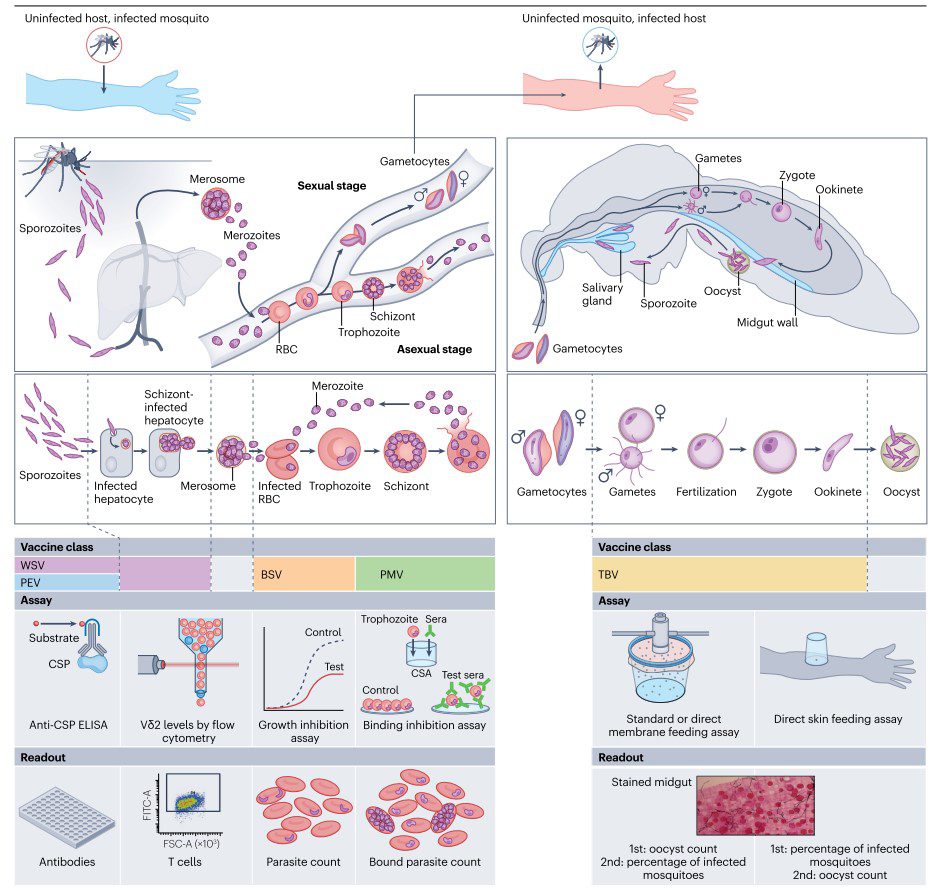
Plasmodium falciparum is the most virulent species of malaria parasites, responsible for the majority of severe and fatal malaria cases globally. P. falciparum is predominantly found in sub-Saharan Africa, but also exists in parts of Southeast Asia, Oceania, and South America. The parasite’s complex life cycle involves anopheline mosquito vectors and human hosts, with key stages including the liver (pre-erythrocytic) stage and the blood (erythrocytic) stage. Its rapid multiplication and the ability to evade immune detection contribute to its pathogenicity and the severity of the diseaseDespite significant global efforts, P. falciparum remains a major public health challenge, necessitating ongoing research and intervention strategies, including the development of effective vaccines and therapies. P. falciparum undergoes several stages in its life cycle. Vaccines target these stages to either prevent infection, reduce symptoms, or block transmission.
Pre-erythrocytic Stage:
- Targets: Sporozoites (infectious form injected by mosquitoes) and liver stages (hepatic schizonts).
- Vaccine Strategy: Prevent the parasite from infecting liver cells and reaching the bloodstream.
- Examples:
- CSP (Circumsporozoite Protein): Major surface protein of sporozoites.
- TRAP (Thrombospondin-related Adhesive Protein): Involved in sporozoite motility and liver cell invasion.
- Liver-stage antigens (LSA-1, LSA-3): Expressed during the liver stage.
Erythrocytic Stage:
- Targets: Merozoites (released from liver cells) and infected red blood cells (erythrocytes).
- Vaccine Strategy: Reduce parasite replication and alleviate symptoms.
- Examples:
- MSP1 (Merozoite Surface Protein 1): Important for red blood cell invasion.
- AMA1 (Apical Membrane Antigen 1): Involved in erythrocyte invasion.
- EBA175 (Erythrocyte Binding Antigen 175): Critical for binding to red blood cells.
- GLURP (Glutamate-rich Protein): Involved in immune evasion.
Transmission-blocking Stage:
- Targets: Sexual stages (gametocytes) and mosquito stages (ookinetes).
- Vaccine Strategy: Prevent the parasite from being transmitted from humans to mosquitoes.
- Examples:
- Pfs25: Surface protein of zygotes and ookinetes.
- Pfs48/45: Gametocyte surface protein.
- Pfs230: Gamete surface protein.
- AnAPN1: Anopheles alanyl aminopeptidase N, involved in midgut invasion by the ookinete.
Pre-erythrocytic Stage Vaccines
RTS,S/AS01 (Mosquirix) Vaccine
The RTS,S/AS01 (Mosquirix) vaccine is a groundbreaking development in the fight against malaria, marking the first time a malaria vaccine has been licensed for widespread use. Its implementation, particularly in sub-Saharan Africa, has shown potential in reducing malaria incidence among young children. Continued research and development efforts aim to improve vaccine efficacy and durability, contributing to the global goal of malaria eradication.
Licensure
- First Licensure: In 2015, the European Medicines Agency (EMA) provided a positive scientific opinion under Article 58, recommending the RTS,S/AS01 malaria vaccine for use in young children in sub-Saharan Africa.
- WHO Pilot Program: In 2019, the World Health Organization (WHO) launched a pilot implementation program in Ghana, Kenya, and Malawi to evaluate the vaccine’s feasibility, safety, and impact in real-world settings.
- Approval: Based on data from the pilot program, RTS,S/AS01 received broader approval for use in endemic regions.
Overview
- Target: The circumsporozoite protein (CSP) of Plasmodium falciparum.
- Adjuvant: AS01, a proprietary adjuvant system designed to enhance the immune response.
- Formulation: The RTS,S vaccine combines a portion of CSP with the hepatitis B surface antigen (HBsAg) to enhance immunogenicity, using AS01 to boost the immune response further.
Clinical Evaluation
- Phase I/II Trials:
- Objective: Assess safety and immunogenicity.
- Population: Conducted in both adults and children.
- Results: Demonstrated that the vaccine was safe and generated a strong immune response.
- Phase IIb Trials:
- Objective: Assess efficacy and further safety.
- Population: Infants and young children in malaria-endemic regions of Africa.
- Results: Showed promising efficacy in reducing malaria episodes.
- Phase III Trials:
- Scale: Conducted in 7 African countries, involving over 15,000 children aged 6 weeks to 17 months.
- Objective: Confirm efficacy, safety, and immunogenicity on a large scale.
- Results:
- Efficacy: Around 39% reduction in clinical malaria episodes over four years in young children. Efficacy against severe malaria was around 29%.
- Safety: Generally well-tolerated with a safety profile comparable to other pediatric vaccines. Common side effects included fever, pain at the injection site, and general malaise.
- Longevity: Efficacy waned over time, highlighting the need for a booster dose to sustain protection.
Significance
- Historical Milestone: RTS,S/AS01 is the first malaria vaccine to be licensed and used on a large scale, representing a major milestone in malaria control efforts.
- Target Population: Specifically aimed at young children in sub-Saharan Africa, where the burden of malaria is highest.
- Impact: RTS,S/AS01 has shown potential in reducing the incidence of malaria and severe malaria, contributing to efforts to decrease the disease burden.
R21/Matrix-M Vaccine
As of April 2023, the R21/Matrix-M malaria vaccine received licensure from Ghana’s Food and Drugs Authority. This is a significant milestone, making R21/Matrix-M another licensed malaria vaccine alongside RTS,S/AS01 (Mosquirix). Here’s a more detailed overview of the R21/Matrix-M vaccine and its development:
Overview
- Target: Circumsporozoite Protein (CSP) of Plasmodium falciparum, similar to RTS,S/AS01.
- Adjuvant: Matrix-M, an adjuvant designed to enhance the immune response.
- Formulation: R21/Matrix-M is formulated with a higher antigen dose compared to RTS,S.
Clinical Trials
- Pre-licensure Trials:
- Phase I/II Trials: Early trials demonstrated safety and strong immunogenicity, prompting further studies.
- Phase IIb Trials: Conducted in Burkina Faso, these trials showed a high efficacy rate. In children aged 5-17 months, the vaccine demonstrated an efficacy of 77% over a 12-month follow-up period.
- Phase III Trials: Large-scale trials were conducted to further confirm efficacy and safety. These trials included thousands of children and showed consistent protection over multiple seasons.
- Results:
- Safety: The vaccine was well-tolerated with a safety profile similar to other pediatric vaccines.
- Efficacy: High efficacy, with substantial protection against clinical malaria episodes.
Licensing
- Ghana: In April 2023, the R21/Matrix-M vaccine was licensed by Ghana’s Food and Drugs Authority. This marked the first national regulatory approval for R21/Matrix-M.
- Subsequent Approvals: Following Ghana’s lead, other countries may consider the vaccine for licensure, especially in regions heavily burdened by malaria.
Significance
- Complement to RTS,S: The licensure of R21/Matrix-M provides an additional tool in the fight against malaria, complementing RTS,S. The higher efficacy reported in trials makes it a promising candidate for broader implementation.
- Manufacturing and Distribution: Efforts are underway to ensure that the vaccine is produced at scale and distributed to regions most in need. Partnerships with organizations like the Serum Institute of India are crucial for this endeavor.
PfSPZ Vaccine (Sanaria)
Overview
- Target: Plasmodium falciparum sporozoites.
- Formulation: Live, attenuated sporozoites delivered intravenously.
- Manufacturer: Sanaria Inc.
Licensure
- Current Status: As of now, PfSPZ has not yet received licensure but has shown promising results in clinical trials and is moving toward large-scale efficacy studies that could lead to eventual approval.
Clinical Evaluation
- Phase I Trials:
- Objective: Assess safety, tolerability, and immunogenicity.
- Population: Conducted in both malaria-naïve adults in the U.S. and in malaria-exposed adults in Africa.
- Results: Demonstrated that the vaccine was safe and well-tolerated. It induced strong immune responses, particularly when administered intravenously.
- Phase II Trials:
- Objective: Assess efficacy and further safety.
- Population: Included malaria-exposed populations in Africa (e.g., Mali and Kenya) and malaria-naïve populations.
- Results: Showed varying levels of protection depending on the dosage and regimen. For example:
- In Mali: The vaccine provided significant protection against malaria infection during the high transmission season.
- In Kenya: Demonstrated up to 100% efficacy in preventing malaria infection in controlled human malaria infection (CHMI) studies.
- Phase III Trials:
- Objective: Confirm large-scale efficacy, safety, and immunogenicity.
- Population: Ongoing trials are assessing the vaccine in different demographic and epidemiological settings, including children and adults in malaria-endemic areas.
- Status: These trials are designed to support eventual licensure by providing comprehensive data on the vaccine’s efficacy and safety profile in larger populations.
Vaccine Mechanism
- Immunization Route: Intravenous administration has been shown to be the most effective delivery method, ensuring that the attenuated sporozoites reach the liver where they elicit an immune response.
- Immune Response: Induces robust CD8+ T cell responses and antibody responses that target the liver stage of the parasite, preventing it from reaching the bloodstream and causing symptomatic malaria.
Significance
- Innovative Approach: PfSPZ represents a novel approach by using whole, attenuated sporozoites, which can potentially offer broad protection across different strains of Plasmodium falciparum.
- High Efficacy: Early trials have shown high levels of protection, particularly in controlled settings, making it a strong candidate for further development.
- Target Population: Aimed at providing protection to both malaria-naïve and malaria-exposed populations, including travelers, military personnel, and residents in endemic regions.
PfSPZ-CVac (Chemoprophylaxis with PfSPZ Vaccine)
Overview
- Target: Plasmodium falciparum sporozoites combined with antimalarial drugs.
- Formulation: Live, non-attenuated sporozoites administered alongside chemoprophylactic agents.
- Manufacturer: Sanaria Inc.
Clinical Evaluation
- Phase I Trials:
- Objective: Assess safety, tolerability, and immunogenicity of the combined approach.
- Population: Conducted in both malaria-naïve and malaria-exposed individuals.
- Results: Showed that the combination of PfSPZ with antimalarial drugs is safe and induces a robust immune response.
- Phase II Trials:
- Objective: Assess efficacy in preventing malaria infection.
- Population: Included malaria-naïve adults in controlled human malaria infection (CHMI) settings and naturally exposed populations.
- Results: Demonstrated high levels of protection. For example, a study showed that PfSPZ-CVac provided up to 100% protection against CHMI with certain dosing regimens.
- Future Trials:
- Objective: Larger trials to confirm efficacy, safety, and feasibility in broader populations and real-world settings.
- Status: Planned or ongoing trials will further evaluate the long-term protection and practical implementation strategies.
Vaccine Mechanism
- Immunization Route: Typically involves intravenous administration of live sporozoites followed by chemoprophylactic drugs to prevent clinical disease.
- Immune Response: Elicits strong T cell and antibody responses against the liver stage of the parasite. The chemoprophylactic drugs ensure that the sporozoites do not cause disease while still promoting an immune response.
Significance
- Innovative Strategy: Combines live sporozoites with chemoprophylaxis to enhance immune protection and potentially provide longer-lasting immunity.
- High Efficacy: Early trials have shown nearly complete protection in some settings, suggesting strong potential for both individual protection and broader public health impact.
- Target Population: Suitable for both endemic regions and travelers, offering flexibility in application based on regional malaria transmission dynamics.
Erythrocytic Stage Vaccines
- PfRH5:
- Target: RH5 protein, essential for red blood cell invasion.
- Mechanism: Induces antibodies that inhibit parasite invasion.
- Clinical Trials:
- Phase I/II: Demonstrated safety and immunogenicity, ongoing trials to assess efficacy.
- MSP3:
- Target: Merozoite surface protein 3.
- Mechanism: Induces antibodies that opsonize merozoites, facilitating their destruction by immune cells.
- Clinical Trials:
- Phase I/II: Showed promising immunogenicity and partial efficacy.
- AMA1:
- Target: Apical membrane antigen 1.
- Mechanism: Induces antibodies that block merozoite invasion of red blood cells.
- Clinical Trials:
- Phase I/II: Demonstrated immunogenicity but variable efficacy due to strain-specific responses.
- EBA175:
- Target: Erythrocyte binding antigen 175.
- Mechanism: Critical for red blood cell invasion.
- Clinical Trials:
- Phase I/II: Trials are ongoing to evaluate safety and efficacy.
- GLURP:
- Target: Glutamate-rich protein.
- Mechanism: Involved in immune evasion.
- Clinical Trials:
- Phase I/II: Early trials indicated immunogenicity.
Transmission-blocking Vaccines
- Pfs25:
- Target: Zygote and ookinete surface protein.
- Mechanism: Induces antibodies that prevent parasite development in the mosquito midgut.
- Clinical Trials:
- Phase I: Showed safety and immunogenicity.
- Phase II: Ongoing to assess efficacy.
- Pfs48/45:
- Target: Gametocyte surface protein.
- Mechanism: Induces antibodies that block fertilization.
- Clinical Trials:
- Phase I/II: Demonstrated safety and immune response.
- Pfs230:
- Target: Gamete surface protein.
- Mechanism: Induces antibodies that block parasite transmission to mosquitoes.
- Clinical Trials:
- Phase I: Ongoing trials to evaluate safety and immune response.
- AnAPN1:
- Target: Anopheles alanyl aminopeptidase N.
- Mechanism: Prevents midgut invasion by the ookinete.
- Clinical Trials:
- Phase I: Initial trials are assessing safety and immunogenicity.
Detailed Clinical Trials Summary
- Phase I Trials:
- Aim: Assess safety and immunogenicity in a small group of volunteers.
- Examples: PfSPZ Vaccine, Pfs25, PfRH5, AMA1.
- Results: Generally show safety and a positive immune response.
- Phase II Trials:
- Aim: Further evaluate safety, immunogenicity, and preliminary efficacy in a larger group.
- Examples: RTS,S/AS01 showed moderate efficacy; R21/Matrix-M showed high efficacy; MSP3 and EBA175 showed mixed results.
- Results: Variable efficacy and immunogenicity, with some candidates showing promising results and others needing further optimization.
- Phase III Trials:
- Aim: Confirm efficacy and monitor side effects in large-scale trials.
- Examples: RTS,S/AS01 was conducted in 7 African countries involving over 15,000 children, leading to licensure.
- Results: Confirmed moderate efficacy and safety, leading to the approval of RTS,S/AS01.
Challenges and Future Directions
- Efficacy and Duration: Current vaccines like RTS,S provide partial protection that diminishes over time, necessitating booster doses.
- Strain Diversity: Plasmodium falciparum exhibits genetic diversity, which can impact vaccine effectiveness. Research is ongoing to develop vaccines that target conserved regions of the parasite.
- Combination Approaches: Future strategies may involve combining different vaccine types (pre-erythrocytic, erythrocytic, and transmission-blocking) to enhance overall protection.
- Novel Targets: Continued research is identifying new targets, such as RH5 for erythrocytic stages and additional transmission-blocking candidates.
Conclusion
Ongoing research and development are crucial to overcoming these challenges, with the ultimate goal of achieving long-lasting, high-efficacy malaria vaccines. This comprehensive approach aims to significantly reduce the global burden of malaria, moving towards eventual eradication.
Vaccines against Plasmodium vivax
Plasmodium vivax is one of the major species causing malaria in humans, with significant public health impacts, particularly in Asia, Latin America, and parts of Africa. Developing an effective vaccine against P. vivax has been challenging due to several factors, including its genetic diversity, complex life cycle, and unique biological features such as the ability to form dormant liver stages (hypnozoites). This summary covers the current status of vaccine development against P. vivax, including the key candidates, targeted stages of the parasite’s life cycle, and clinical trials.
Pre-Erythrocytic Stage Vaccines
These vaccines aim to target the parasite before it reaches the blood stage, primarily focusing on the sporozoite and liver stages.
- CSP-based Vaccines: Similar to P. falciparum, P. vivax circumsporozoite protein (PvCSP) is a major target. PvCSP is involved in sporozoite invasion of hepatocytes.
- VMP001: A vaccine candidate composed of a recombinant chimeric protein representing portions of PvCSP. It has been evaluated in clinical trials for its ability to induce immune responses against sporozoites.
- Clinical Trials: Phase I trials have shown that VMP001 is safe and immunogenic, inducing antibodies against PvCSP.
- Whole Sporozoite Vaccines: Utilizing attenuated or inactivated whole sporozoites to induce immunity.
- Preclinical and Early Clinical Research: These studies are ongoing to evaluate the feasibility of using whole sporozoites for P. vivax vaccination.
Blood Stage Vaccines
These vaccines target the merozoite stage, aiming to prevent the parasite’s invasion of red blood cells, thereby reducing the severity of disease and transmission.
- Merozoite Surface Protein 1 (PvMSP1): A key target for blood-stage vaccines, as MSP1 plays a crucial role in merozoite invasion of red blood cells.
- PvMSP1-19: A subunit vaccine candidate based on the 19-kDa C-terminal fragment of MSP1.
- Clinical Trials: PvMSP1-19 has been tested in early-phase clinical trials, showing safety and the ability to elicit an immune response.
- Duffy Binding Protein (PvDBP): Critical for the parasite’s invasion of red blood cells by interacting with the Duffy antigen receptor.
- Vaccine Candidates: Several vaccine candidates based on PvDBP have been developed, aiming to block this interaction and prevent erythrocyte invasion.
- Clinical Trials: Early-phase trials have demonstrated immunogenicity and safety, though challenges remain due to genetic polymorphism in PvDBP.
Transmission-Blocking Vaccines (TBVs)
TBVs target the sexual stages of the parasite, aiming to block transmission from humans to mosquitoes, thereby reducing the spread of malaria.
- Pvs25 and Pvs28: Proteins expressed on the surface of zygotes and ookinetes in the mosquito midgut.
- Vaccine Candidates: Candidates targeting Pvs25 and Pvs28 have been developed to generate antibodies that block parasite development in the mosquito.
- Clinical Trials: Early-phase clinical trials have tested the safety and immunogenicity of Pvs25-based vaccines, showing promise in inducing transmission-blocking antibodies.
Clinical Trials and Developmental Challenges
Clinical Evaluation
- Safety and Immunogenicity: Most P. vivax vaccine candidates have undergone Phase I trials, which primarily assess safety and the ability to induce an immune response.
- Efficacy Trials: Phase II and III trials are more challenging to conduct due to the lower prevalence of P. vivax in certain regions and the need for larger cohorts to demonstrate efficacy.
- Challenges in P. vivax Vaccine Development
- Hypnozoite Stage: The ability of P. vivax to form dormant liver stages (hypnozoites) that can cause relapses is a unique challenge. There is no effective vaccine target identified for this stage as of now.
- Genetic Diversity: High genetic diversity, especially in antigens like PvDBP, complicates vaccine design and effectiveness.
- Duffy-Negative Populations: A significant portion of the population in sub-Saharan Africa is Duffy-negative, which traditionally provides protection against P. vivax. However, recent reports of P. vivax infections in these populations complicate vaccine target selection.
- Co-infection and Cross-Species Immunity: The co-circulation of different Plasmodium species can complicate the interpretation of immune responses and vaccine efficacy.
Future Directions
- Multistage and Multi-antigen Approaches: Developing vaccines that target multiple stages of the parasite’s life cycle and multiple antigens could improve efficacy and provide broader protection.
- Innovative Platforms: Exploring new vaccine platforms such as viral vectors, mRNA vaccines, and nanoparticle-based vaccines.
- Global Partnerships and Trials: Increased collaboration among research institutions, public health organizations, and governments to facilitate large-scale clinical trials and ensure equitable access to vaccines.
- Monitoring and Surveillance: Implementing robust systems for monitoring vaccine efficacy and potential escape variants in diverse geographical settings.
Conclusion
The development of vaccines against Plasmodium vivax malaria is an ongoing and challenging endeavor. While several candidates targeting different stages of the parasite’s life cycle have shown promise in early clinical trials, significant hurdles remain. The complexity of P. vivax biology, including the hypnozoite stage and genetic diversity, necessitates continued research and innovative approaches to develop a highly effective vaccine. Collaboration and commitment across global health stakeholders are crucial for advancing these efforts and ultimately achieving a significant reduction in the burden of P. vivax malaria.